国家报告文书(2024年)
Background
2010年第六十三届世界卫生大会(WHA63.16号决议)通过的《世界卫生组织全球卫生人员国际招聘行为守则》(以下简称《守则》)意在加强数据、信息和国际合作,从而加强对卫生人员国际招聘的了解和道德管理。
《守则》第7条鼓励世卫组织会员国交换与卫生人员国际招聘和移民有关的信息。根据授权,世卫组织总干事每三年向世界卫生大会提交一次报告。
世卫组织会员国已于2022年5月完成第四轮国家报告。世卫组织总干事已于2022年5月向第七十五届世界卫生大会报告了《守则》的执行进展情况(A75/14)。 第四轮报告强调,在COVID-19大流行导致脆弱性增加的背景下,有必要评估卫生人员向国外移民所产生的影响。为此,重新召集了《守则》相关性和有效性专家咨询小组(A73/9)。根据专家咨询小组的建议,秘书处公布了 “2023年世卫组织卫生人力支持和保障措施受益国名单”。
本国家报告文书是一个以国家为基础、用于信息交流和监测《守则》执行情况的自评工具。它使世卫组织能够收集和分享关于卫生人员国际招聘和移民的现有证据和信息。第五轮国家报告的结果将于2025年1月提交执行委员会(执委会第一五六届会议),以便为举行第七十八届世界卫生大会做准备。
提交报告的截止日期为2024年8月31日。
《守则》第9条授权世卫组织总干事定期向世界卫生大会报告对《守则》在实现其既定目标方面的有效性的审查情况,并提出改进建议。世卫组织将在2024年召集一个由会员国牵头的专家咨询小组,以便对《守则》进行第三次审查。审查报告将提交第七十八届世界卫生大会。
如对填写在线问卷有任何疑问或需要说明,请通过 WHOGlobalCode@who.int与我们联系。
什么是世卫组织《全球卫生人员国际招聘行为守则》?
免责声明: 通过国家报告文书收集的数据和信息将在第七十八届世界卫生大会之后通过国家报告文书数据库(https://www.who.int/teams/health-workforce/migration/practice/reports-database)公开提供。定量数据将用于为国家卫生人力账户数据门户网站(http://www.apps.who.int/nhwaportal/)提供信息。
Disclaimer
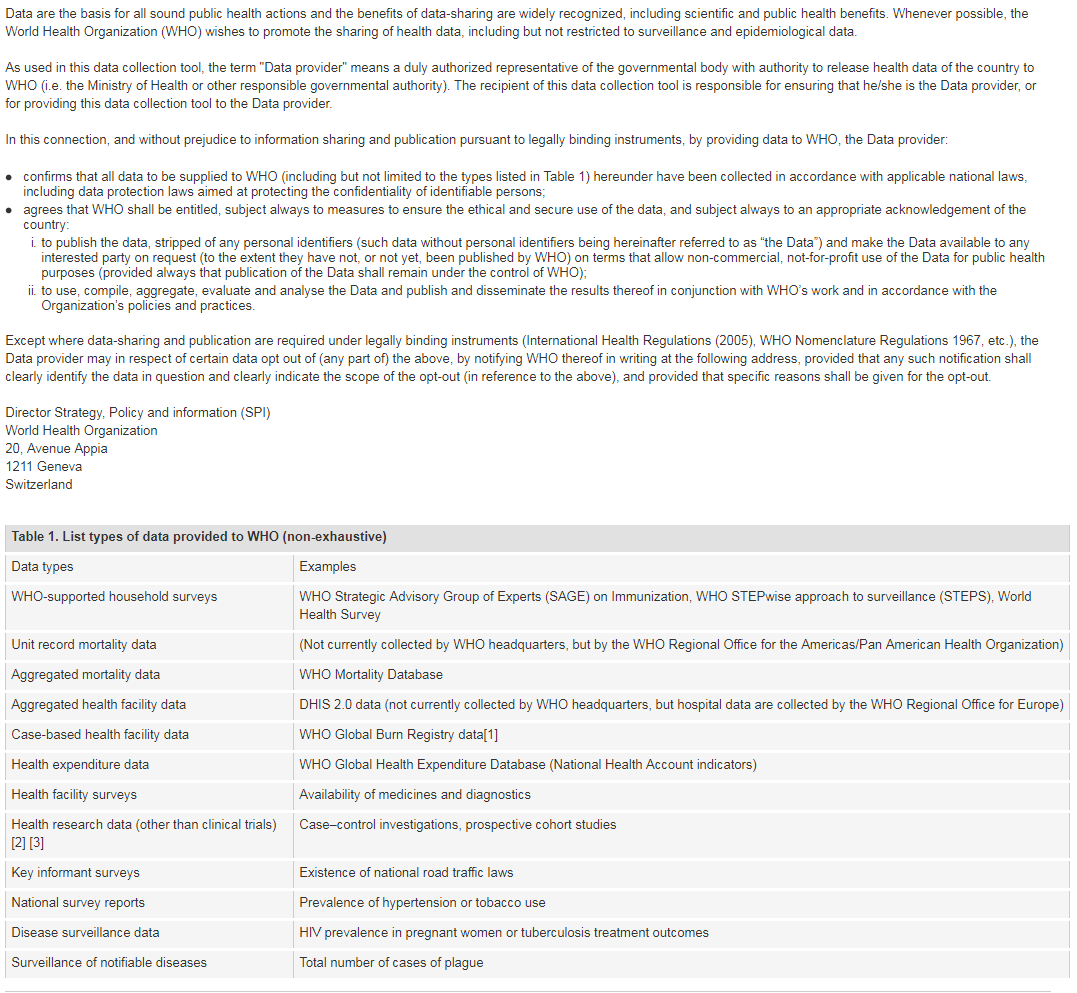
[1] Note: Case-based facility data collection as that in the WHO Global Bum Registry does not require WHO Member State approval.
[2] The world health report 2013: research for universal coverage. Geneva: World Health Organization; 2013 (http://apps.who.int/iris/bitstream/10665/85761/2/9789240690837_eng.pdf)
[3] WHO statement on public disclosure of clinical trial results: Geneva: World Health Organization; 2015 (http://www.who.int/ictrp/results/en/, accessed 21 February 2018).
For more information on WHO Data Policy kindly refer to http://www.who.int/publishing/datapolicy/en/
Contact Details
Contemporary issues
Norway relies on its citizens pursuing education abroad, particularly in the fields of medicine and dentistry, to meet the nation's needs for those groups. Additionally, Norway sees a steady arrival of healthcare professionals from abroad, including nurses, healthcare workers, and doctors. Most of these professionals come from the Nordic countries or the EU/EEA. Therefore monitoring of domestic educational capacity is crucial to ensure that Norway continues to have a robust healthcare workforce.
Health Personnel Education
Government Agreements
Responsibilities, rights and recruitment practices
请从下面列表中勾选所有适用选项:
请从下面列表中勾选所有适用选项:
International migration
| 直接(个人)申请教育、就业、贸易、移民或入境. | 允许卫生人员流动的政府间协议 | 私人招聘机构或雇主协助招聘 | 私人教育/移民咨询机构协助流动 | 其它途径(请具体说明) | 哪一种途径用得最多?如有数据资料,请提供。 | |
|---|---|---|---|---|---|---|
| 医生 | 1 | 0 | 1 | 0 | Direct | |
| 护士 | 1 | 0 | 1 | 0 | Direct | |
| 助产士 | 1 | 0 | 1 | 0 | Direct | |
| 牙医 | 1 | 0 | 1 | 0 | Direct | |
| 药剂师 | 1 | 0 | 1 | 0 | Direct | |
| 其它专业 | 1 | 0 | 1 | 0 | Direct | |
| 其它专业 | 1 | 0 | 1 | 0 | Direct | |
| 其它专业 | 0 | 0 | 0 | 0 | ||
| 其它专业 | 0 | 0 | 0 | 0 | ||
| 其它专业 | 0 | 0 | 0 | 0 |
| 直接(个人)申请教育、就业、贸易、移民或入境目的地国 | 允许卫生人员流动的政府间协议 | 私人招聘机构或雇主协助招聘 | 私人教育/移民咨询机构协助流动 | 其它(请具体说明) | 哪一种途径用得最多? 如有数据资料,请提供。 | |
|---|---|---|---|---|---|---|
| 医生 | 1 | 0 | 0 | 0 | Direct | |
| 护士 | 1 | 0 | 0 | 0 | Direct | |
| 助产士 | 1 | 0 | 0 | 0 | Direct | |
| 牙医 | 1 | 0 | 0 | 0 | Direct | |
| 药剂师 | 1 | 0 | 0 | 0 | Direct | |
| 其它专业 | 1 | 0 | 0 | 0 | Direct | |
| 其它专业 | 0 | 0 | 0 | 0 | ||
| 其它专业 | 0 | 0 | 0 | 0 | ||
| 其它专业 | 0 | 0 | 0 | 0 | ||
| 其它专业 | 0 | 0 | 0 | 0 |
Recruitment & migration
增加数据的可用性和国际可比性对于了解和应对卫生工作者移民的全球动态至关重要。请与贵国卫生人力账户联络点(如有)进行咨询,以确保以下报告的数据与国家卫生人力账户报告一致*。
(关于贵国国家卫生人力账户联络点的详细信息,请参见电子版国家报告文书或联系WHOGlobalCode@who.int)
Inflow and outflow of health personnel
| 医生 | 护士 | 助产士 | 牙医 | 药剂师 | 备注 | |
|---|---|---|---|---|---|---|
| 2021 | ||||||
| 2022 | ||||||
| 2023 | ||||||
| 数据来源(如监管机构、移民记录、工作许可证等) |
| 医生 | 护士 | 助产士 | 牙医 | 药剂师 | 备注 | |
|---|---|---|---|---|---|---|
| 2021 | ||||||
| 2022 | ||||||
| 2023 | ||||||
| 数据来源(例如有良好信誉的信函、移民记录、政府间协议等) |
Stock of health personnel
请根据国家卫生人力账户指标1-07和1-08提供有可用数据的最新一年的资料,以说明贵国按培训地(在外国培训)和出生地(在外国出生)分列的卫生人员(最好是在职卫生人员)的总储备人数。
这一信息可通过以下两个选项中的一个提供:
Technical and financial support
| 支持的国家 | 支持类型(请具体说明) | |
|---|---|---|
| Ethiopia, Tanzania, Zanzibar, Ghana and Nepal | Health system strengthening – capacity for priority setting – through University of Bergen | |
| Ethiopia, Tanzania, Ghana and Nepal | Health System Strengthening - non-communicable diseases – through University of Bergen/WHO | |
| 80 LMICs | Health System Strengthening – DHIS2 - through University of Oslo | |
| Malawi | Health System Strengthening – Broad bilateral sector support. |
| 支持的国家: | 支持领域: | 支持类型: | |
|---|---|---|---|
| Malawi, Palestine, Ghana, Nepal, Africa CDC | Building Stronger Public Health Institutions and Systems | Bilateral, Technical Assistance | |
| Malawi, Zambia, Zimbabwe | Improve access to sports for all | Triangular, strengthening of institutions | |
Constraints, Solutions, and Complementary Comments
| 主要制约因素 | 可能的解决办法/建议 | |
|---|---|---|
| A considerable share of the healthcare workforce in Norway has received their training abroad, including a significant number of Norwegians. This highlights a somewhat dependency on internationally trained staff. This reliance became particularly evident during the pandemic. | In addition to enhancing educational capacity and completion rates in certain professions, efforts must also be made to make employment in the healthcare sector more attractive. This could involve improving working conditions, more full-time employment, and providing opportunities for professional development. Such initiatives can help to retain skilled workers and reduce the pull effect from other sectors. | |
| We have reason to believe that municipalities and public-sector hospitals recruit in accordance with the Code, while we know less about the practices of recruitment agencies. These agencies offer personnel to the same municipalities and hospitals, especially during vacations and when they have problems with recruiting. | Recruitment firms could engage more proactively and undergo closer scrutiny. We believe hospitals and local governments are avoiding firms with negative reputations | |
| While migration data are of high quality, we still need more knowledge. For example, we have no data qualitative data about the motivation of migrants, and hence we do not know if the migration is a result of active recruitment. Also, we don't know enough about migration patterns and the extent of the domino effect. | We support further work and are looking at our own opportunities for continued work on strengthening international migration data and research. |
We do not see a need to update the code per se, but this will be useful to discuss in the Expert Advisory Group in the ongoing process of reviewing the relevance and effectiveness of the Code; where the EAG can make use of the WHO Secretariat’s normative mandate and capabilities and seek advice from the Secretariat on which governance options provide the best trade-off between feasibility and potential for a positive impact.
No need to update process, but more important than ever to engage with a broad range of stakeholders and to achieve attention at the highest level