National Reporting Instrument 2024
Background
[INFOxNRI1]
National Reporting instrument 2024
[BGxINT]
Background
Adopted in 2010 at the 63rd World Health Assembly (WHA Res 63.16), the WHO Global Code of Practice on the International Recruitment of Health Personnel (“the Code”) seeks to strengthen the understanding and ethical management of international health personnel recruitment through improved data, information, and international cooperation.
Article 7 of the Code encourages WHO Member States to exchange information on the international recruitment and migration of health personnel. The WHO Director General is mandated to report to the World Health Assembly every 3 years.
WHO Member States completed the 4th round of national reporting in May 2022. The WHO Director General reported progress on implementation to the 75th World Health Assembly in May 2022 (A75/14). The report on the fourth round highlighted the need to assess implications of health personnel emigration in the context of additional vulnerabilities brought about by the COVID-19 pandemic. For this purpose, the Expert Advisory Group on the relevance and effectiveness of the Code (A 73/9) was reconvened. Following the recommendations of the Expert Advisory Group, the Secretariat has published the WHO health workforce support and safeguards list 2023.
The National Reporting Instrument (NRI) is a country-based, self-assessment tool for information exchange and Code monitoring. The NRI enables WHO to collect and share current evidence and information on the international recruitment and migration of health personnel. The findings from the 5th round of national reporting will be presented to the Executive Board (EB156) in January 2025 in preparation for the 78th World Health Assembly.
The deadline for submitting reports is 31 August 2024.
Article 9 of the Code mandates the WHO Director General to periodically report to the World Health Assembly on the review of the Code’s effectiveness in achieving its stated objectives and suggestions for its improvement. In 2024 a Member-State led expert advisory group will be convened for the third review of the Code’s relevance and effectiveness. The final report of the review will be presented to the 78th World Health Assembly.
For any queries or clarifications on filling in the online questionnaire please contact us at WHOGlobalCode@who.int.
What is the WHO Global Code of Practice?
Disclaimer: The data and information collected through the National Reporting Instrument will be made publicly available via the NRI database (https://www.who.int/teams/health-workforce/migration/practice/reports-database) following the proceedings of the 78th World Health Assembly. The quantitative data will be used to inform the National Health Workforce Accounts data portal (http://www.apps.who.int/nhwaportal/).
Adopted in 2010 at the 63rd World Health Assembly (WHA Res 63.16), the WHO Global Code of Practice on the International Recruitment of Health Personnel (“the Code”) seeks to strengthen the understanding and ethical management of international health personnel recruitment through improved data, information, and international cooperation.
Article 7 of the Code encourages WHO Member States to exchange information on the international recruitment and migration of health personnel. The WHO Director General is mandated to report to the World Health Assembly every 3 years.
WHO Member States completed the 4th round of national reporting in May 2022. The WHO Director General reported progress on implementation to the 75th World Health Assembly in May 2022 (A75/14). The report on the fourth round highlighted the need to assess implications of health personnel emigration in the context of additional vulnerabilities brought about by the COVID-19 pandemic. For this purpose, the Expert Advisory Group on the relevance and effectiveness of the Code (A 73/9) was reconvened. Following the recommendations of the Expert Advisory Group, the Secretariat has published the WHO health workforce support and safeguards list 2023.
The National Reporting Instrument (NRI) is a country-based, self-assessment tool for information exchange and Code monitoring. The NRI enables WHO to collect and share current evidence and information on the international recruitment and migration of health personnel. The findings from the 5th round of national reporting will be presented to the Executive Board (EB156) in January 2025 in preparation for the 78th World Health Assembly.
The deadline for submitting reports is 31 August 2024.
Article 9 of the Code mandates the WHO Director General to periodically report to the World Health Assembly on the review of the Code’s effectiveness in achieving its stated objectives and suggestions for its improvement. In 2024 a Member-State led expert advisory group will be convened for the third review of the Code’s relevance and effectiveness. The final report of the review will be presented to the 78th World Health Assembly.
For any queries or clarifications on filling in the online questionnaire please contact us at WHOGlobalCode@who.int.
What is the WHO Global Code of Practice?
Disclaimer: The data and information collected through the National Reporting Instrument will be made publicly available via the NRI database (https://www.who.int/teams/health-workforce/migration/practice/reports-database) following the proceedings of the 78th World Health Assembly. The quantitative data will be used to inform the National Health Workforce Accounts data portal (http://www.apps.who.int/nhwaportal/).
Disclaimer
[INFOxNRI2]
National Reporting instrument 2024
[disclaim]
Disclaimer
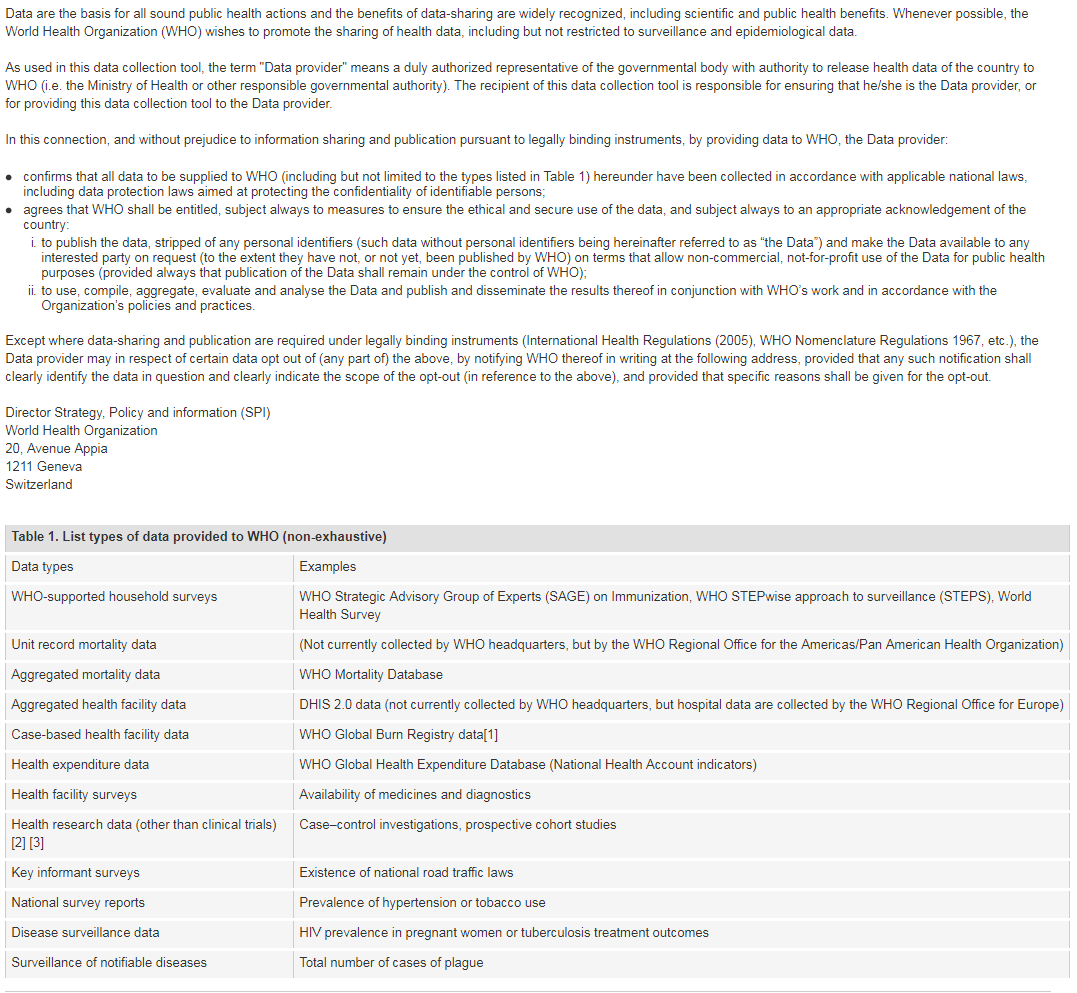
[1] Note: Case-based facility data collection as that in the WHO Global Bum Registry does not require WHO Member State approval.
[2] The world health report 2013: research for universal coverage. Geneva: World Health Organization; 2013 (http://apps.who.int/iris/bitstream/10665/85761/2/9789240690837_eng.pdf)
[3] WHO statement on public disclosure of clinical trial results: Geneva: World Health Organization; 2015 (http://www.who.int/ictrp/results/en/, accessed 21 February 2018).
For more information on WHO Data Policy kindly refer to http://www.who.int/publishing/datapolicy/en/
[1] Note: Case-based facility data collection as that in the WHO Global Bum Registry does not require WHO Member State approval.
[2] The world health report 2013: research for universal coverage. Geneva: World Health Organization; 2013 (http://apps.who.int/iris/bitstream/10665/85761/2/9789240690837_eng.pdf)
[3] WHO statement on public disclosure of clinical trial results: Geneva: World Health Organization; 2015 (http://www.who.int/ictrp/results/en/, accessed 21 February 2018).
For more information on WHO Data Policy kindly refer to http://www.who.int/publishing/datapolicy/en/
I have read and understood the WHO policy on the use and sharing of data collected by WHO in Member States outside the context of public health emergencies
Contact Details
[INFOxNRI3]
National Reporting instrument 2024
[CI]
Contact Details
Name of Member State:
Sweden
Name of designated national authority:
Jesper Sellerburg
Title of designated national authority:
Programme Officer
Institution of the designated national authority:
Socialstyrelsen
Email:
riginao@who.int,Jesper.Sellerberg@socialstyrelsen.se,WHOGlobalCode@who.int
Telephone number :
Contemporary issues
[INFOxNRI4]
National Reporting instrument 2024
[NRIxI]
The questions marked * are mandatory. The system will not allow submission until all mandatory questions are answered.
[INFOx1]
Contemporary issues on health personnel migration and mobility
[Q1x1]
In the past 3 years, has the issue of international recruitment of health personnel been a concern for your country?
No, this is not a problem in my country
[Q1x2]
In the past 3 years, has the issue of international reliance on health personnel (international recruitment of health personnel to meet domestic needs) been a concern for your country?
No, this is not a problem in my country
Health Personnel Education
[INFOxNRI5]
National Reporting instrument 2024
[INFOx2]
Health personnel education, employment and health system sustainability
[Q2]
Is your country taking measures to educate, employ and retain a health and care workforce that is appropriate for the specific conditions of your country, including areas of greatest need?
Yes
[Q2x1]
Please check all items that apply from the list below:
2.1 Measures taken to ensure the sustainability of the health and care workforce
2.2 Measures taken to address the geographical mal-distribution and retention of health and care workers*
2.3 Other relevant measures taken to educate, employ and retain a health and care workforce that is appropriate for the specific conditions of your country
[Q2x1x1]
2.1.1 Measures taken to ensure the sustainability of the health and care workforce
Forecasting future health and care workforce requirements to inform planning
Government agencies, Socialstyrelsen among them, together share data and publish reports containing statistical analysis and forecasting of health care needs in relation till available workforce and for example rate of examination from various health care education programmes.
Aligning domestic health and care workforce education with health system needs
Improving quality of education and health personnel in alignment with service delivery needs
Creating employment opportunities aligned with population health needs
Managing international recruitment of health personnel
Improving management of health personnel
Specific provisions on health personnel regulation and recruitment during emergencies
Others
[Q3x1]
Are there specific policies and/or laws that guide international recruitment, migration and integration of foreign-trained health personnel in your country?
Yes
[Q3x1x1]
Please provide further information in the box below:
Law/policy 1
Socialstyrelsens föreskrifter och allmänna råd (HSLF-FS 2016:64) om erkännande av yrkeskvalifikationer
Law/policy 2
Socialstyrelsens föreskrifter och allmänna råd (HSLF-FS 2017:80) om legitimation och annat behörighetsbevis vid utbildning från tredjeland
Law/policy 3
[Q3x2]
Are there any policies and/or provision for international telehealth services in your country through health personnel based abroad?
No
[Q3x3]
Has your country established a database or compilation of laws and regulations related to international health personnel recruitment and migration and, as appropriate, information related to their implementation?
No
[Q4]
Recognizing the role of other government entities, does the Ministry of Health have mechanisms (e.g. policies, processes, unit) to monitor and coordinate across sectors on issues related to the international recruitment and migration of health personnel?
Yes
[Q4x1]
Please describe
In Sweden, each government agency is under the responsibility of a specific ministry. The The Ministry of Health and Social Affairs is responsible for issues concerning social welfare, such as public health, health care and care of older people. The National Board of Health and Welfare (Socialstyrelsen) is the agency which is monitered under the Ministry of Health and Social Affairs. The Ministry of Health and Social Affairs also coordinates with the Ministry of Foreign Affairs and the Ministry of Employment. Socialstyrelsen, and other government agencies also coordinate and share data with each other for a number of tasks, including international recruitment and migration of health personnel.
[Q5]
Please describe the steps taken by your country to implement the following Code recommendations.
Check all items that apply from the list below:
Check all items that apply from the list below:
5.1 Measures have been taken or are being considered to introduce changes to laws or policies on health personnel consistent with the recommendations of the Code.
5.2 Actions have been taken to communicate and share information across
sectors on the international recruitment and migration of health personnel, as well as to publicize the Code, among relevant ministries, departments and agencies,
nationally and/or sub-nationally.
sectors on the international recruitment and migration of health personnel, as well as to publicize the Code, among relevant ministries, departments and agencies,
nationally and/or sub-nationally.
5.3 Measures have been taken to consult stakeholders in decision-making
processes and/or involve them in activities related to the international recruitment of health personnel.
processes and/or involve them in activities related to the international recruitment of health personnel.
5.4 Records are maintained on all private recruitment agencies for health
personnel authorized by competent authorities to operate within their jurisdiction.
personnel authorized by competent authorities to operate within their jurisdiction.
5.5 Good practices, as called for by the Code, are encouraged and promoted among private recruitment agencies.
5.5a Promotion of the Code among private recruitment agencies.
5.5b Domestic legislation or policy requiring ethical practice of private recruitment agencies, as consistent with the principles and articles of the Code.
5.5c Public or private certification of ethical practice for private recruitment agencies.
5.5d Others
5.6 None of the above
Socialstyrelsen handles the application process to become certfied among all health care professions that require a license to practice. As such, the code is implemented at the agency (Socialstyrelsen) to be applied during the application process.
Government Agreements
[INFOxNRI6]
National Reporting instrument 2024
[INFOx3]
Government-to-Government agreements on migration or mobility of health personnel
[Q6]
Has your country or sub-national governments entered into any bilateral, multilateral, or regional agreements and/or arrangements with respect to the international recruitment and/or mobility of health personnel?
No
Responsibilities, rights and recruitment practices
[INFOxNRI9]
National Reporting instrument 2024
[INFOx4]
Responsibilities, rights and recruitment practices
[Q7]
If your country employs/hosts international health personnel to work in the health and care sectors, which legal safeguards and/or other mechanisms are in place for migrant health personnel and to ensure that enjoy the same legal rights and responsibilities as the domestically trained health workforce?
Please check all items that apply from the list below:
Please check all items that apply from the list below:
Migrant health personnel are recruited using mechanisms that allow them to assess the benefits and risk associated with employment positions and to make timely and informed decisions on the employment.
Migrant health personnel are hired, promoted and remunerated based on objective criteria such as levels of qualification, years of experience and degrees of professional responsibility on the same basis as the domestically trained health workforce.
Migrant health personnel enjoy the same opportunities as the domestically trained health workforce to strengthen their professional education, qualifications and career progression.
Institutional arrangements are in place to ensure safe migration/ mobility and integration of migrant health personnel.
Measures have been taken to promote circular migration of international health personnel
Other measures (including legal and administrative) for fair recruitment and employment practices of foreign-trained and/or immigrant health personnel (please provide details)
No measures in place
Not applicable – does not host/employ foreign health personnel
[Q8]
If health personnel from your country are working abroad in the health and care sectors, please provide information on measures that have been taken or are planned in your country to ensure their fair recruitment and employment; safe migration; return; and diaspora utilization in your country, as well as difficulties encountered.
Please check all items that apply from the list below:
Please check all items that apply from the list below:
Arrangements for fair recruitment
Arrangements for decent employment contracts and working conditions in destination countries
Arrangements for safe mobility
Arrangements for return and reintegration to the health labour market in your country
Arrangements for diaspora engagement to support your country health system
Other
No measures in place
No specific arrangements exists, and instead the laws of the other country, as well as EU-regulations on working permits.
Not applicable – health personnel from my country are not working abroad
International migration
[INFOxNRI10]
National Reporting instrument 2024
[INFOx5]
International migration and mobility pathways for health personnel
[Q9x1]
9.1 If your country hosts international health personnel to work in the health and care sector, how do they come to your country? (check all that apply)
| Direct (individual) application for education, employment, trade, immigration or entry in country |
Government to government agreements that allow health personnel mobility |
Private recruitment agencies or employer facilitated recruitment |
Private education/ immigration consultancies facilitated mobility |
Other pathways (please specify) | Which pathway is used the most? Please include quantitative data if available. | |
|---|---|---|---|---|---|---|
| Doctors | 1 | 1 | 0 | 0 | ||
| Nurses | 1 | 0 | 0 | 0 | ||
| Midwives | 1 | 0 | 0 | 0 | ||
| Dentists | 1 | 1 | 0 | 0 | ||
| Pharmacists | 1 | 0 | 0 | 0 | ||
| Other occupations | 0 | 0 | 0 | 0 | ||
| Other occupations | 0 | 0 | 0 | 0 | ||
| Other occupations | 0 | 0 | 0 | 0 | ||
| Other occupations | 0 | 0 | 0 | 0 | ||
| Other occupations | 0 | 0 | 0 | 0 |
[Q9x1oth]
The same applies for all 22 professions that require a license to practice
[Q9x2]
9.2 If health personnel from your country work/study abroad, how do they leave your country?
(check all that apply)
| Direct (individual) application for education, employment, trade, immigration, or entry in the destination country |
Government to government agreements that allow health personnel mobility |
Private recruitment agencies or employer facilitated recruitment |
Private education/ immigration consultancies facilitated mobility |
Other pathways (please specify) | Which pathway is used the most? Please include quantitative data if available. | |
|---|---|---|---|---|---|---|
| Doctors | 1 | 1 | 0 | 0 | ||
| Nurses | 1 | 0 | 0 | 0 | ||
| Midwives | 1 | 0 | 0 | 0 | ||
| Dentists | 1 | 1 | 0 | 0 | ||
| Pharmacists | 1 | 0 | 0 | 0 | ||
| Other occupations | 1 | 0 | 0 | 0 | ||
| Other occupations | 0 | 0 | 0 | 0 | ||
| Other occupations | 0 | 0 | 0 | 0 | ||
| Other occupations | 0 | 0 | 0 | 0 | ||
| Other occupations | 0 | 0 | 0 | 0 |
[Q9x2oth]
The same applies for all 22 professions that require a license to practice
Recruitment & migration
[INFOxNRI11]
National Reporting instrument 2024
[INFOx6]
Data on international health personnel recruitment & migration
Improving the availability and international comparability of data is essential to understanding and addressing the global dynamic of health worker migration. Please consult with your NHWA focal point, if available, to ensure that data reported below is consistent with NHWA reporting*.
(The list of NHWA focal points is available here. Please find the focal point(s) for your country from the list and consult with them.)
For countries reporting through the WHO-Euro/EuroStat/OECD Joint data collection process, please liaise with the JDC focal point.
[Q10]
Does your country have any mechanism(s) or entity(ies) to maintain statistical records of foreign-born and foreign-trained health personnel?
Yes
[Q10x1]
Where are the records maintained? (check all that apply)
Employment records or work permits
Ministry of health personnel database
Registry of health personnel authorized to practice
Other
[Q10x1x1]
Please specify:
Details on origin of EU/EES personnel are in the registry, while the origin of third country personnel are archived in the license applications.
[Q10x2]
Does the record include gender-disaggregated data on the foreign-born and/or foreign-trained health personnel?
Yes
Inflow and outflow of health personnel
[INFOxNRI12]
National Reporting instrument 2024
[INFOx7]
Inflow and outflow of health personnel
[Q11]
Do you have a mechanism to monitor the inflow and outflow of health personnel to/from your country? (check all that apply)
Inflow
Outflow
No
[Q11xI]
If yes for inflow:
Fill in the table below
[Q11x1]
How many foreign-trained or foreign-born health personnel were newly active (temporarily and/or permanently) in your country in the past three years (inflow)?
| Doctors | Nurses | Midwives | Dentists | Pharmacists | Remarks | |
|---|---|---|---|---|---|---|
| 2021 | 532 | 164 | 10 | 68 | 23 | The data refers to November, 2021. Source: Licensed Care and Welfare Personnel Workforce Status register |
| 2022 | ||||||
| 2023 | ||||||
| Data Source (e.g. Regulatory authority, immigration records, work permits, etc.) |
[Q11xO]
If yes for outflow:
Fill in the table below
[Q11x2]
How many domestically trained health personnel left your country in the past years for temporary or permanent migration (outflow)?
| Doctors | Nurses | Midwives | Dentists | Pharmacists | Remarks | |
|---|---|---|---|---|---|---|
| 2021 | 58 | 155 | 12 | 18 | 13 | The data refers to November, 2021. Source: Licensed Care and Welfare Personnel Workforce Status register |
| 2022 | ||||||
| 2023 | ||||||
| Data Source (e.g. letters of good standing, emigration records, government to government agreements etc.) |
[Q11x3]
If you have any document with information on health worker inflows and outflows for your country, please upload
Stock of health personnel
[INFOxNRI13]
National Reporting instrument 2024
[INFOx8]
Stock of health personnel
[Q12x1]
Consolidated stock on health personnel, disaggregated by place of training and birth
For the latest year available, consistent with the National Health Workforce Accounts (NHWA) Indicators 1-07 and 1-08, please provide information on the total stock of health personnel in your country (preferably the active workforce), disaggregated by the place of training (foreign-trained) and the place of birth (foreign-born).
For the latest year available, consistent with the National Health Workforce Accounts (NHWA) Indicators 1-07 and 1-08, please provide information on the total stock of health personnel in your country (preferably the active workforce), disaggregated by the place of training (foreign-trained) and the place of birth (foreign-born).
[Q12x1a]
Please provide data on the stock of active health personnel in your country by one of the following ways:
Fill in the table below
[Q12x1x1]
| Medical Doctors (generalist + specialists) | 42627 | 27579 | 9130 | 28215 | 14406 | The data refers to November, 2021. Source: Licensed Care and Welfare Personnel Workforce Status register | 2021 | 1 | |||
| Nurses | 114596 | 110379 | 2597 | 100548 | 14045 | The data refers to November, 2021. Source: Licensed Care and Welfare Personnel Workforce Status register | 2021 | 1 | |||
| Midwives | 8015 | 6597 | 186 | 7139 | 876 | The data refers to November, 2021. Source: Licensed Care and Welfare Personnel Workforce Status register | 2021 | 1 | |||
| Dentists | 8066 | 6223 | 883 | 5090 | 2976 | The data refers to November, 2021. Source: Licensed Care and Welfare Personnel Workforce Status register | 2021 | 1 | |||
| Pharmacists | 8146 | 7059 | 378 | 5187 | 2959 | The data refers to November, 2021. Source: Licensed Care and Welfare Personnel Workforce Status register | 2021 | 1 |
[Q12x1x1x]
If you have any document with information on stock of active health personnel for your country, their distribution by place of training and place of birth, please upload
[Q12x2]
Please provide data on the top 10 countries of training for foreign-trained health personnel in your country.
This information can be provided by one of the following two options:
This information can be provided by one of the following two options:
Fill in the table below
[Q12x2x1]
| Doctors | Nurses | Midwives | Dentists | Pharmacists | |
|---|---|---|---|---|---|
| Total foreign trained personnel | 9130 | ||||
| Country 1: Top country of training | POL | ||||
| Country 1: No. of foreign trained health personnel | 1415 | ||||
| Country 2: Top country of training | ROU | ||||
| Country 2: No. of foreign trained health personnel | 1136 | ||||
| Country 3: Top country of training | DEU | ||||
| Country 3: No. of foreign trained health personnel | 941 | ||||
| Country 4: Top country of training | |||||
| Country 4: No. of foreign trained health personnel | |||||
| Country 5: Top country of training | |||||
| Country 5: No. of foreign trained health personnel | |||||
| Country 6: Top country of training | |||||
| Country 6: No. of foreign trained health personnel | |||||
| Country 7: Top country of training | |||||
| Country 7: No. of foreign trained health personnel | |||||
| Country 8: Top country of training | |||||
| Country 8: No. of foreign trained health personnel | |||||
| Country 9: Top country of training | |||||
| Country 9: No. of foreign trained health personnel | |||||
| Country 10: Top country of training | |||||
| Country 10: No. of foreign trained health personnel | |||||
| Source (e.g. professional register, census data, national survey, other) | Licensed Care and Welfare Personnel Workforce Status register | Licensed Care and Welfare Personnel Workforce Status register | Licensed Care and Welfare Personnel Workforce Status register | Licensed Care and Welfare Personnel Workforce Status register | Licensed Care and Welfare Personnel Workforce Status register |
| Year of data (Please provide the data of the latest year available) | 2021 | 2021 | 2021 | 2021 | 2021 |
| Remarks | The table only includes the countries in the EU/EES-area. Data on personnel from other countries are unknown. | The table only includes the countries in the EU/EES-area. Data on personnel from other countries are unknown. | The table only includes the countries in the EU/EES-area. Data on personnel from other countries are unknown. | The table only includes the countries in the EU/EES-area. Data on personnel from other countries are unknown. | The table only includes the countries in the EU/EES-area. Data on personnel from other countries are unknown. |
[Q12x2x1x]
If you have any document with information on the distribution of foreign-trained health personnel for your country by their country of training, please upload
Sweden NRI 12.2

The session always expires and I cannot fill out the table in the survey.
Technical and financial support
[INFOxNRI14]
National Reporting instrument 2024
[INFOx9]
Technical and financial support
[Q13]
Has your country provided technical or financial assistance to any source countries or countries in the WHO health workforce support and safeguards list 2023, or other low- and middle-income countries on health workforce development, health system strengthening, or for implementing other recommendations of the Code (e.g., strengthening data, information and research on health workforce for translation to policies and planning, etc.)
No
[Q14]
Has your country received technical or financial assistance from any WHO Member State or other stakeholders (e.g., development partners, other agencies) for health workforce development, health system strengthening, or for implementing other recommendations of the Code (e.g., strengthening data, information and research on health workforce for translation to policies and planning, etc.)?
No
Constraints, Solutions, and Complementary Comments
[INFOxNRI15]
National Reporting instrument 2024
[INFOx10]
Constraints, Solutions, and Complementary Comments
[Q15]
Please list in priority order, the three main constraints to the ethical management of international migration in your country and propose possible solutions:
| Main constraints | Possible solutions/recommendations | |
|---|---|---|
[Q16]
What support do you require to strengthen implementation of the Code?
Support to strengthen data and information on health personnel
Support for policy dialogue and development
Support for the development of bilateral/multi-lateral agreements
There is a chain effect regarding international recruitment. For example, even if Sweden does not have a large stock of international recruitments from countries on the safe guard list, there is no way to know to what extent our recruitment from e.g. Germany and Poland has on their respective recruitments from countries on the list.
Others
No support required
[Q17]
Considering that the Code is a dynamic document that should be updated as required, please provide reflections from your country on the past 14 years since the resolution on the Code.
[Q17x1]
Please comment on if/how the Code has been useful to your country.
The code is useful and Sweden is determined to upheld the code in mutual relations with other countries. See comment above. Sweden cannot assure that recruitment from a country that is not on the safe guard list doesn't affect those countries in a chain reaction type of situation. This would be up to the WHO to follow up and provide data on. Otherwise it is difficult for one single country to upheld the code.
[Q17x2]
Do any articles of the Code need to be updated?
No
[Q17x3]
Does the process of reporting on Code implementation and the review of the Code relevance and effectiveness need to be updated?
Yes
I couldn't fill out table 12.2 within time for the survey to expire.
[Q17x4]
Please comment on the WHO health workforce support and safeguards list (e.g. if your country is included in the list, how has that affected you; if your country is reliant on international health personnel, how has the list affected you; if your country is not in the list, how has it affected you)
See comments above regarding chain reaction recruitment practices.
[Q18]
Submit any other complementary comments or material you may wish to provide regarding the international recruitment and migration of health personnel, as related to implementation of the Code.
Please describe OR Upload (Maximum file size 10 MB)
Please describe OR Upload (Maximum file size 10 MB)
See comments above regarding chain reaction recruitment practices.
[Q18x1]
Warning
[INFOxNRI16]
National Reporting instrument 2024
[WARN]
You have reached the end of the National Reporting Instrument - 2024. You may go back to any question to update your answers or confirm your entry by clicking ‘Submit’.