
Health data management for before, during and after emergencies and disasters - Health data collection tools
Data collection is the systematic process of gathering, compling, managing and analysing different types of information from multiple sources [1]. To provide the full picture of ongoing issues and a foundation for efficient decision-making and research, good quality data should be collected in standadised manner [2].
However, collecting and sharing health data in emergencies is often a challnge [3]. Evidence from a literature review funded by WHO Kobe Centre (WKC) identified key barriers to effective data collection and analysis, such as a lack of standardised systems for collecting, sharing and storing data, a lack of clear guidance, limited collaboration between stakeholders, a lack of trained personnel, and unreliable infrastructure [4].
To tackle these challenges, various standardised data collection approaches and tools have been developed and implemented at national, regional and global level. The WHO Health EDRM Knowledge Hub on Health Data Management introduces 3 data collection tools in emergencies: 1. Emergency Medical Team Menimum Data Set (EMT MDS), 2. Early Warning Alert and Response System (EWARS), and 3. Japan Surveillance in Post Extreme Emergencies and Disasters (J-SPEED).
1. Emergency Medical Team Menimum Data Set (EMT MDS)
During emergencies, external health professionals may provide extra health services in disaster affected areas [5]. The WHO Emergency Medical Team (EMT) initiative was developed after the 2010 Haiti earthquake, aiming to improve the timeliness and quality of health services provided by national and international Emergency Medical Teams (EMTs) and to increase capacity of national health systems in leading the activation and coordination of EMT response [5].
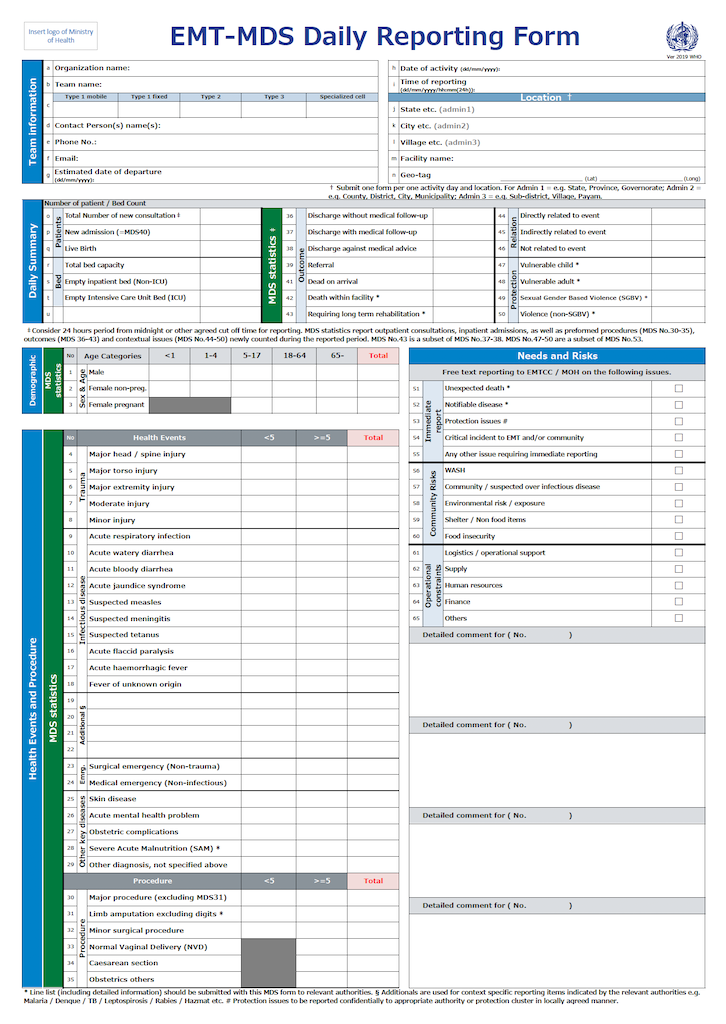
For EMTs to obtain essential and standardised data for implementing efficient and coordinated responses in emergency situations, WHO developed a standardised medical data collection tool, the Emergency Medical Team Minimum Data Set (EMT MDS), in 2017 to gather essential information during EMT consultations [6]. The EMT MDS uses a daily reporting form to collect 85 items in four categories during EMT consultations [6]:
Category 1: Team Information (14 items): e.g. name of organisations
Category 2: Daily Summary (6 items): e.g. the total number of consultations, new admissions, total bed capacity
Category 3: MDS Statistics (50 items): sex, age, health events, (e.g.trauma, infectious disease, emergency)
Category 4: Needs and Risks (15 items): e.g. community risks, operational constraints
The WHO EMT MDS has been used in multiple disasters and conflict situations. The case study under a WKC research project on ‘Health data collection during emergency and disaster (2020-2021)' describes how WHO EMT MDS was used during Cyclone Idai in Mozambique in 2019.
|
Case Study 1: Tropical Cyclone Idai, Mozambique, 2019 [6] The EMT MDS daily form was introduced during Cyclone Idai in Mozambique in 2019 and captured 18,468 medical consultations in the 110-days period of the EMT response. The data collected in the consultations were statistically analysed. The major finding included two most frequently reported conditions: minor injuries and acute watery diarrhoea. These findings helped to develop the most effective resource allocation plan for managers. This research also identified that staff training on how to complete the form was important for acquisition of accurate data. Read more. |
2. Early Warning Alert and Response System (EWARS)
The WHO’s Early Warning Alert and Response System (EWARS) was established to address the need for good quality and real-time data for timely detection and response to epidemics in emergency settings, such as in countries in conflict or following a natural disaster [7].
EWARS uses ‘EWARS in a box’ which contains all the equipment needed to gather data for surveillance and response activities in difficult and remote field settings without reliable internet or electricity. WHO provides an online training package for ‘EWARS in a box’ which provides a comprehensive overview of establishing EWARS in a box in the field with the key features and functionalities of the tool.
Data are entered at the facility level and automatically uploaded into a central database. The results could be rapidly achieved through automated analysis and be disseminated to all health partners on a regular basis [8]. The EWARS not only generates data for public health decision making during humanitarian crises, but also serving as foundation for strengthening disease surveillance during the transition from humanitarian to development programming. Moreover the system is a major repository of secondary research data.
|
Case Study 2: EWARS in a human-made disaster in Sub-Saharan Africa [9] An armed conflict in Sub-Saharan Africa internally displaced more than one million people into camps who were predisposed to increased risk of infectious diseases due to poor living conditions and reduced access to social services [10]. South Sudan’s Ministry of Health officially confirmed a cholera outbreak and a total of 1160 cholera cases including 23 deaths were reported between July and August 2016. The majority of cases were found in Juba County, where an average of 35 new admissions were recorded daily. The data collected by EWARS contributed to tracking cholera cases and led to a more targeted response to cholera outbreaks, such as implementing oral cholera vaccines in community centres where cholera outbreaks are expected to rise [7]. The system resulted in improvements in the timeliness and completeness of reporting from the camps and conflict-affected locations [9]. This case study was referred from Chapter 4.2: Measuring the problem: Basic statistics. in the WHO Guidance on Research Methods for Health Emergency and Disaster Risk Management, revised 2022. |
3. Japan-Surveillance in Post-Extreme Emergencies and Disasters (J-SPEED)
The Japan-Surveillance in Post-Extreme Emergencies and Disasters (J-SPEED) is a national standard data collection and reporting tool in Japan to collect near real-time health data during emergencies and disasters [3]. J-SPEED uses a standard daily reporting form to gather data such as the number of patients and type of health problems complained during medical consultations by the EMTs. J-SPEED reporting form can be accessed from mobile applications or website and data can be directly typed in. [3].
The J-SPEED system has been used in multiple health emergency situations in Japan since 2016. The 3 case studies under a WKC research project on ‘Health data collection during emergency and disaster (2020-2021)' show you how standardised health data can reveal.
|
Case Study 3: Earthquake, Hokkaido, 2018 [11] J-SPEED data captured 739 consultations in the 32-day period of the EMT response in the 2018 Hokkaido Earthquake and 97.6% of consultations occurred in the first 2 weeks. Most consultations were with people over 65 years old and women. Disaster stress related symptoms were the most frequently reported health condition (15.2%), followed by wounds (14.5%) and skin diseases (7.0%). Read more. |
|
Case Study 4: Heavy rain, West Japan, 2018 [12] During the 2018 West Japan heavy rain event, J-SPEED collected health data from 3,617 medical consultations in the 65-day period of the EMT response. A descriptive analysis of the data revealed that the majority of patients were between 15 and 64 years old. Skin disease was the most frequently reported health event (17.3%), followed by wounds (14.3%), disaster stress-related symptoms (10.0%), conjunctivitis (6.3%), and acute respiratory infections (5.4%). Read more. |
|
Case Study 5: A comparison study: Incidence of Acute Respiratory Infections during Disasters in the Absence and Presence of COVID-19 Pandemic [13] This comparative study investigated if there were any differences in acute respiratory infection (ARI) incidence in the absence and presence of COVID-19 Pandemic, by comparing J-SPEED data obtained in the two heavy rain disasters in Japan; West Japan in 2018 and Kumamoto in 2020. The result showed that the ARI incident rates were 5.4% of the total consultation in the 2018 West Japan heavy rain (before COVID-19) and 1.2% in the 2020 Kumamoto heavy rain (during COVID-19) (P <.001). The researchers concluded that the significant reduction in the ARI incidence rate in the 2020 Kumamoto heavy rain event could be due to the COVID-19 preventive measures implemented at personal and organizational level, such as wearing masks, disinfecting hands, maintaining social distance, improving room ventilation, and screening at evacuation centres. Read more. |
More information
More information on health data collection and management can be found in Chapter 4.4: Collection and management of good quality data in the WHO Guidance on Research Methods for Health Emergency and Disaster Risk Management, revised 2022.
References
[1] WHO. (2022). The role of Emergency Medical Teams in the health response to the Ukraine war. https://www.who.int/europe/news/item/02-06-2022-the-role-of-emergency-m… (Accessed 24 Feb 2023)
[2] Gouvew-Reis F, Dell'Aringa MF, Murray V. Chapter 4.4 Collection and management of good quality data. In: WHO Guidance on Research Methods for Health Emergency and Disaster Risk Management, revised 2022. World Health Organization; 2022: 271-281. https://apps.who.int/iris/handle/10665/363502 (accessed 15 June 2023).
[3] Kubo T, Yanasan A, Herbosa T, Buddh N, Fernando F, Kayano R. Health Data Collection Before, During and After Emergencies and Disasters-The Result of the Kobe Expert Meeting. Int J Environ Res Public Health. 2019 Mar 12;16(5):893. doi: 10.3390/ijerph16050893. PMID: 30871037; PMCID: PMC6427760.
[4] JHU scoping review
[5] WHO. The WHO Emergency Medical Team (EMT) initiative. https://www.who.int/emergencies/partners/emergency-medical-teams (Accessed 20 May 2023)
[6] Kubo T, Chimed-Ochir O, Cossa M, Ussene I, Toyokuni Y, Yumiya Y, Kayano, R, and Salio, F. (2022). First Activation of the WHO Emergency Medical Team Minimum Data Set in the 2019 Response to Tropical Cyclone Idai in Mozambique. Prehospital and Disaster Medicine, 37(6), 727-734. doi:10.1017/S1049023X22001406
[7] South Sudan health crisis worsens. WHO. 2016. https://www.who.int/news-room/feature-stories/detail/south-sudan-health… (accessed 15 June 2023)
[8] Early Warning Alert and Response in Emergencies: an operational guide. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO.
[9] Orach CG, Nsenga N, Olu O, Harris M. Chapter 4.2: Measuring the problem: Basic statistics. In: WHO Guidance on Research Methods for Health Emergency and Disaster Risk Management, revised 2022. World Health Organization; 2022: 271-281. https://apps.who.int/iris/handle/10665/363502 (accessed 15 June 2023).
[10] Outbreak surveillance and response in humanitarian emergencies. WHO. 2012. http://www.who.int/diseasecontrol_emergencies/ publications/who_hse_epr_dce_2012.1/en/ (accessed 15 June 2023).
[11] Yumiya Y, Chimed-Ochir O, Kayano R, Hitomi Y, Akahoshi K, Kondo H, Wakai A, Mimura S, Chishima K, Toyokuni Y, Koido Y, and Kubo T. (2023). Emergency Medical Team Response during the Hokkaido Eastern Iburi Earthquake 2018: J-SPEED Data Analysis. Prehospital and Disaster Medicine, 1-6. doi:10.1017/S1049023X23000432
[12] Chimed-Ochir O, Yumiya Y, Taji A, Kishita E, Kondo H, Wakai A, Akahoshi K, Chishima K, Toyokuni Y, Koido Y, Kubo T. Emergency Medical Teams' Responses during the West Japan Heavy Rain 2018: J-SPEED Data Analysis. (2022). Prehosp Disaster Med. 28;37(2):1-7. doi:10.1017/S1049023X22000231. Epub ahead of print. PMID: 35225205; PMCID: PMC8958047.
[13] Sugimura M, Chimed-Ochir O, Yumiya Y, Taji A, Kishita E, Tsurugi Y, Kiwaki K, Wakai A, Kondo H, Akahoshi K, Chishima K, Toyokuni Y, Koido Y, Kubo T. Incidence of Acute Respiratory Infections during Disasters in the Absence and Presence of COVID-19 Pandemic. (2022). Prehosp Disaster Med. 11:1-10. doi: 10.1017/S1049023X22000085. Epub ahead of print. PMID: 35012691.